
The Expectancy Effect and Age-Related Macular Degeneration Research: A Scoping Review
By Corinna Trujillo Tanner, Michael Caserta, Lisa M. Ord, Paul S. Bernstein, Julia Kleinschmidt, Margaret Clayton, and Jia-Wen Guo
Corinna Trujillo Tanner, Ph.D., RN, is an assistant professor at Brigham Young University.
Michael Caserta is a professor in the College of Nursing at the University of Utah.
Lisa M. Ord is an associate professor of ophthalmology and visual sciences at the University of Utah.
Paul S. Bernstein is a professor of ophthalmology and visual sciences at the University of Utah.
Julia Kleinschmidt is professor emeritus of ophthalmology and visual sciences at the University of Utah.
Margaret Clayton is a professor in the College of Nursing at the University of Utah.
Jia-Wen Guo is an assistant professor in the College of Nursing at the University of Utah.
Acknowledgement: We wish to acknowledge the excellent efforts of our research assistant Adam Palmer
Abstract
According to Rosenthal’s expectancy effect, our conscious and unconscious attitudes and expectations may impact the behaviors of those around us. A loss-focused paradigm may affect understanding of the potential of individuals with age-related macular degeneration (AMD), their self-expectations, and their outcomes. Thus, we undertook a scoping review according to the five-stage framework proposed by Arksey and O’Malley (2005). The purpose was to provide a comprehensive overview of the relevant research related to how researchers study and report the effects of AMD on individuals, families, caregivers, and communities. The review links findings to negative perceptions of blindness, including the hierarchy of sight. Findings are discussed in the context of Rosenthal’s expectancy effect. Gaps in the literature are identified, with recommendations for future research. Results indicate that there is a strong negative bias and loss focus in the existing literature. Scientific inquiry into the psychological, health, and social issues surrounding AMD has focused on its negative outcomes. This body of literature has emerged out of a sociocultural environment that may have influenced the questions asked about vision loss and the outcomes expected. This could affect research findings and patient outcomes. Reframing expected outcomes from the struggle with blindness may include investigating positive outcomes, such as posttraumatic growth (PTG). The positive influence of low-vision rehabilitation and blindness training should not be ignored.
“One of the most devastating things that can happen to any human being is to be trapped in the prison of low expectations.” (Omvig, 2004)
Keywords
Expectancy effect, age-related macular degeneration, behavior, scoping review
Introduction
As the leading cause of irreversible blindness worldwide, age-related macular degeneration (AMD) may profoundly affect individuals, families, caregivers, and communities (National Eye Institute, n.d.; World Health Organization, n.d.). Rein et al. (2009) estimated that after including the effects of new AMD treatments in an agent-based simulation model, there would be large increases in the number of people with both early (from 9.1 to 17.8 million) and late (from 620,000 to 1.6 million) AMD over the next 40 years, owing to the aging of the U.S. population.
Research literature documents many losses that accompany the onset of vision loss and blindness. These include loss of mobility, including driving privileges (Chan, Fujiyama, & Rubin, 2015; Owsley & McGwin, 2008); difficulty with activities of daily living and visually intensive tasks, such as reading print (Bennion, Shaw, & Gibson, 2012; Lamoureux, Hassell, & Keeffe, 2004; Weih, Hassell, & Keeffe, 2002; West et al., 1997); significant reduction in participation in social activities (Vu, Keeffe, McCarty, & Taylor, 2005); reduction in participation in religious activities (West et al., 2002); and significantly increased risk of falls and hip fracture (with accompanying mortality; Chung, Hu, Lin, Kao, & Huang, 2017; Ivers, Cumming, Mitchell, Simpson, & Peduto, 2003). Persons with AMD may also experience increases in reliance on community support resources (Bennion et al., 2012; Wang, Mitchell, Smith, Cumming, & Attebo, 1999), use of health-care resources (Brown et al., 2016; Meyer-Ruesenberg & Richard, 2010), rate of institutionalization (Wang, Mitchell, Cumming, & Smith, 2003), and emotional distress and depressive symptoms (Casten & Rovner, 2013; Chung, Ho, Hwa, Lee, & Lin, 2015; Wang, Mitchell, & Smith, 2000). The consensus seems to be that the negative impact of vision loss is profound and comes at a high personal and societal cost (Brown et al., 2016; Kuyk et al., 2008; Marback, Maia, Morais, & Takahashi, 2007; Vu et al., 2005).
Although older adults with vision loss may be at increased risk for experiencing devastating losses, these losses are not inevitable. Low-vision rehabilitation, which may include training in the use of tactile cues, training in video magnification and low-vision aids, and organizational strategies help older adults to improve their function and maintain their independence (Kaldenberg, 2019). Additional compensatory skills can be learned that greatly mitigate or reverse functional losses: training in the nonvisual use of computers, audible reading, braille reading, travel training, and orientation and mobility training. Each of these merits discussion in the context of loss. Together, these skills have been shown to protect the quality of life of older adults who have experienced vision loss (Lamoureux et al., 2004; Lamoureux et al., 2007; Teitelman & Copolillo, 2005). The concept that blindness alone imputes negative outcomes, which at face value seems plausible, is misleading when understood in the context of restorative training (Jernigan, 1984).
Hierarchy of sight is a term first defined by blind attorney and activist James Omvig (2002). The term describes the unfounded notion that the better an individual’s visual acuity, the better his or her outcomes in life will be. For example, when referring to older adults with vision loss, according to the hierarchy of sight we assume that the blind individual is more disabled, more depressed, and more socially isolated (and so forth) than his or her sighted peers. This is true only in the absence of rehabilitation and training. Brody et al. (2002), in a randomized controlled trial, found that depression among visually impaired older adults was low when study participants received self-management training and high when they did not. This suggests that it was not low visual acuity that had the biggest impact on depression, but rather access to training. In the best-case scenario, the hierarchy of sight is incomplete, as it ignores the well-founded evidence that blindness rehabilitation is effective and crucial to maintaining independence with blindness. In the worst-case scenario, adherence to the hierarchy of sight is clear evidence of implicit bias toward the blind.
According to Rosenthal’s expectancy effect (Rosenthal & Jacobson, 1966, 1968), researchers’ expectations may affect the findings of their studies because their conscious and unconscious beliefs may guide the questions they ask as well as the outcomes of their studies. The expectancy effect is also demonstrated through the social behaviors that impact others in our sphere of influence, as documented in Rosenthal’s hallmark “Pygmalion in the Classroom” study (Rosenthal & Jacobson, 1968), in which schoolteachers’ unfounded expectations of students profoundly affected their students’ academic performance. Within 10 years of publication of that study, the phenomenon of the expectancy effect was documented in 345 studies in seven domains. In the health care literature, the effects of caregiver expectations on nursing-home-patient clinical outcomes were demonstrated in six nursing-home facilities where newly admitted patients were randomly assigned to a “high-expectations” group or an “average-expectations” group. Nurses and nurses’ aides were informed of these expectations. At the 3-month mark, the initial assessments were performed again (this time by a research assistant with no previous knowledge of categorization of the groups), and the high-expectations group was significantly less depressed and had greater functional independence in comparison to the average-expectations group (Learman, Avorn, Everitt, & Rosenthal, 1990). A research paradigm that documents primarily negative outcomes of vision loss could reflect cultural and societal beliefs about blindness (Conrad, Mackie, & Mehrotra, 2010; Joyce, 2008) and could become a self-fulfilling prophecy for those experiencing vision loss, as negative expectations trickle down from researchers to clinicians, policy makers, or rehabilitation professionals to individuals with visual impairment.
Scoping Review
We undertook a scoping review according to the five-stage framework proposed by Arksey and O’Malley (2005) to provide a comprehensive overview of the relevant research related to the social, psychological, monetary, quality-of-life, and health impact of AMD. While a systematic review might typically focus on a well-defined question whereby appropriate study designs can be identified in advance, a scoping review tends to address broader topics in which many different study designs might be applicable.
Scoping reviews are a relatively new but increasingly common approach to mapping broad topics (Pham et al., 2014). The aim of a scoping review is to map the existing literature in a field of interest in terms of volume, nature, and characteristics (Arksey & O’Malley, 2005). A scoping review of a body of literature can be useful if the topic has not been extensively reviewed or, in the case of this review, if the topic is being analyzed from a new perspective (Mays, Roberts, & Popay, 2001). It differs from other types of reviews, as it may include a heterogeneous collection of literature, including research studies, letters to the editor, conference proceedings, and other works; thus, articles in the review are not typically “scored” but are, rather, described (Arksey & O’Malley, 2005). Scoping reviews are used to identify knowledge gaps and set research agendas (Tricco et al., 2016).
We searched the literature for direct or indirect evidence that negative attitudes and beliefs about AMD and the potential of individuals who have AMD had colored the questions asked in research and the outcomes reported. We did not survey or chart literature surrounding adjustment to AMD, as this construct is disparate from the impact itself, although adjustment and rehabilitation are addressed in relation to removing barriers posed by AMD.
Methods
The scoping review was conducted according to the five-stage process proposed by Arksey and O’Malley (2005): (a) identifying questions; (b) identifying relevant studies; (c) selecting studies to include; (d) charting the data; and (e) collating, summarizing, and reporting. These steps are often performed iteratively, and the questions identified may change as greater familiarity with the literature is achieved (Arksey & O’Malley, 2005).
Identifying questions.
We posed the following initial research questions to guide the search:
- How is the impact of AMD measured? In what light (positive, negative, or neutral) are items in instruments framed?
This is an important question because some instruments and measures assume negative outcomes and estimate only negative outcomes (i.e., the degree to which a loss has occurred). - To what extent are the outcomes of AMD-related vision loss reported as solely negative?
If the primary outcomes reported in a given study are negative, this reinforces a loss-focused paradigm. We are not suggesting that there are not negative outcomes accruing from vision loss; rather, in making these losses central to our research foci and reporting, we risk propagating loss and negative outcomes, as these are the outcomes blindness professionals and others will subsequently expect. - Is there evidence that the study design or reported outcomes reinforced the hierarchy of sight?
This question emerged as we reviewed the full-text articles identified for the scoping study.
Identifying relevant studies.
Arksey and O’Malley (2005) recommended surveying a broad array of literature by employing a wide definition of key words for search terms. Search terms and key concepts were developed to capture the impact of AMD or outcomes of AMD at any level: individual, family, community, or population. Inclusion and exclusion criteria guided article selection and were developed post hoc based on our familiarity with the literature, as proposed by Arksey and O’Malley. We included all peer-reviewed articles reporting quality-of-life and health-related quality-of-life issues for individuals with AMD, as well as those reporting on the psychosocial, financial, and health-related impact associated with AMD, including depression, injury, comorbidities caused by vision loss, negative associations, and positive associations. We also included articles published in peer-reviewed journals, such as state-of-the-science reports, letters to the editor, and case studies. We excluded articles that reported clinical interventions, the psychological process (i.e., adjustment or rehabilitation), quality of life after interventions, prediction of or risk factors for AMD, value or cost-effectiveness of treatment, photodynamics, pharmacodynamics, physiology of the eye, an incorrect diagnosis for something other than AMD, treatments of the retina, and measures or assessments of a psychometric tool. The start date and end dates for the search were left open to capture a broader view of the body of literature and to identify trends in research over time. Foreign-language material was excluded due to the cost and time required for translation (see Table 1).
The researcher and a medical librarian determined appropriate search terms to capture articles based on an iterative process described by Arksey and O’Malley (2005). Final search terms included age-related macular degeneration, AMD, ARMD, depression, anxiety, self-concept, self-awareness, self-efficacy, personal autonomy, social isolation, aptitude, ability, physical mobility, driving ability, independent living, institutionalization, activity, disability, fall, life expectancy, quality of life, health-related quality of life, and activities of daily living. Searches were completed on July 12, 2017 (EMBASE), August 15, 2017 (Ovid/MEDLINE and CINAHL), and August 25, 2017 (PubMed/MEDLINE and Web of Science).
Selecting studies to include.
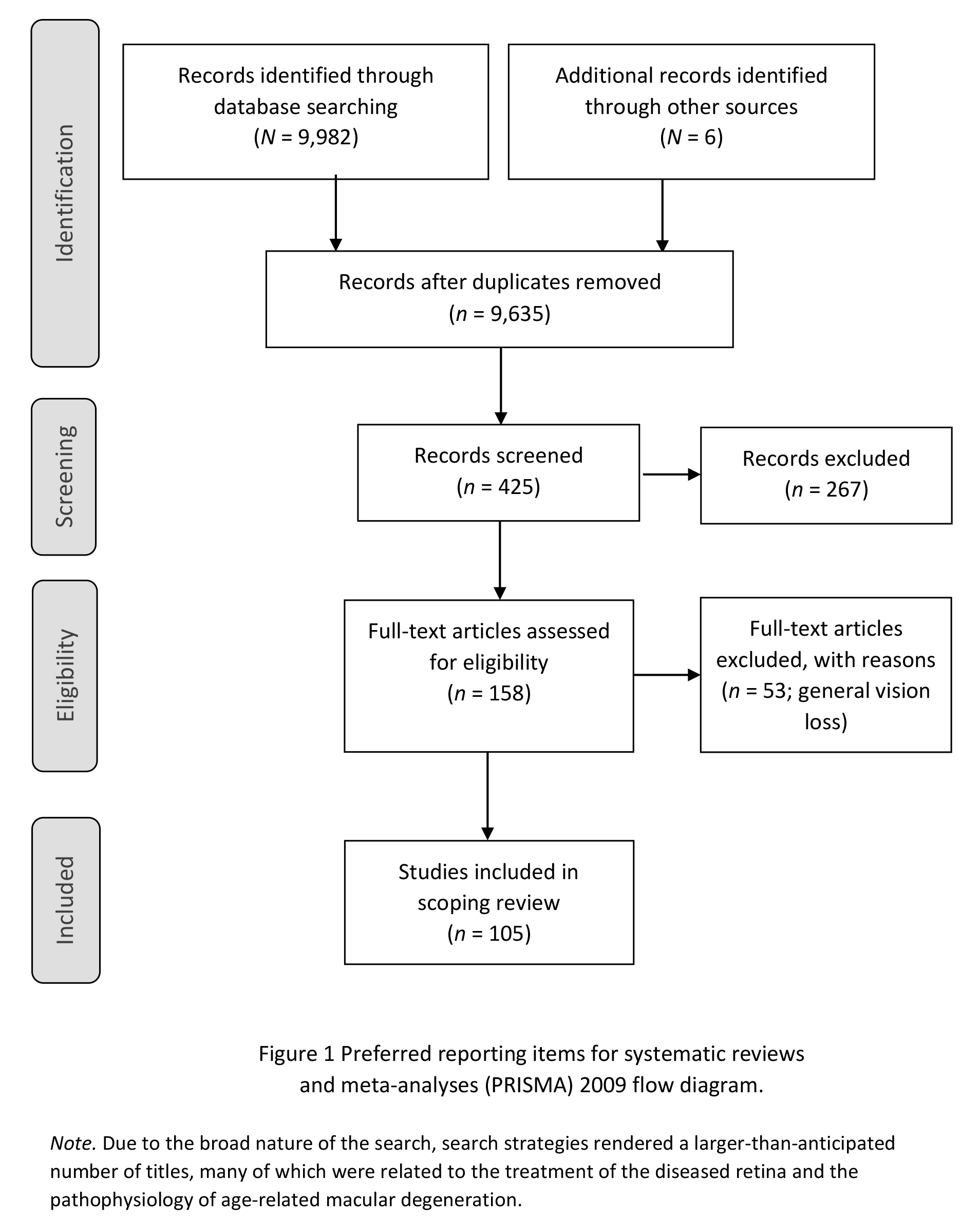
Citations were reviewed in two phases. For the first level of screening, only the titles and abstracts for citations were reviewed, to prevent procuring articles that did not meet minimum inclusion criteria. The process of article selection followed the Preferred Reporting of Items for Systematic Reviews and Meta-analyses flow diagram (Figure 1; Moher, Liberati, Tetzlaff, & Altman, 2009). Citations were reviewed using covidence.org (a Cochran technology platform), a Web-based tool for organizing and conducting literature reviews. Using the key search descriptors, 9,982 titles and abstracts were identified and screened by the researcher; six additional articles were identified and added through reference review. After duplicates were identified and removed, this was refined to 9,635. Due to the broad nature of the search, search strategies rendered a larger-than-anticipated number of titles, many of which were related to the treatment of the diseased retina and the pathophysiology of AMD. Therefore, these were eliminated, and 425 articles remained for full-text review. The full texts of articles were independently read, coded, and screened by two reviewers. Reviewers met regularly throughout the screening process to resolve conflicts and discuss uncertainties regarding study selection, as recommended (Levac, Colquhoun, & O’Brien, 2010). After 267 articles were removed because they did not fit inclusion criteria, a selection of 158 articles was identified. By consensus, the decision was made to include only articles specifically reporting the impact of vision loss caused by AMD and not the impact of vision loss in general; thus, an additional 53 articles were removed and the final number of articles selected for the review was 105 (Figure 1).
Charting the data.
The fourth stage of Arksey and O’Malley’s (2005) scoping-review framework was charting selected articles. Characteristics of the 105 included articles were independently charted by two of the authors and a research assistant using a standardized form, and discrepancies were resolved by discussion. Summaries were created for each article and included year of publication, title, authors, journal, sample size, study design, outcome measures, posture of report of findings (negative outcome, reinforced hierarchy of sight), and study location.
Findings
The final stage of Arksey and O’Malley’s (2005) framework consists of collating, summarizing, and reporting findings, which are presented in this section. Detailed data depicting the key elements and features of each article are presented in Appendix A and summarized in aggregate form in Table 2. Most of the studies (n = 93) were conducted in the United States or the United Kingdom, but the remainder represented 17 countries, reflecting that AMD is of concern worldwide. Studies were published in 52 journals, including eight articles in Investigative Ophthalmology and Visual Science and seven in the British Journal of Ophthalmology. The nature of the journals in which the studies were published varied broadly, including journals focusing on clinical and laboratory science, rehabilitation, nursing, occupational therapy, gerontology, and health economics, which suggests that the impact of AMD is of concern for many. Years of publication ranged from 1988 to 2017, with the bulk of the articles (47) published between 2011 and 2017. This recent increase in interest in the personal and societal impact of AMD may have been spurred by the emergence of AMD treatment modalities (intravitreal antiangiogenic therapy, previously unavailable and now widely used; Jager, Mieler, & Miller, 2008) and breakthrough developments in nutritional therapy for AMD (Jager et al., 2008), because some articles reporting negative outcomes of AMD are used as the rationale for these new treatments. The study design most frequently used to measure the impact of AMD was cross-sectional (n = 69; mean sample size = 333). Other study designs included reviews of literature (n = 15), longitudinal studies (n = 7; mean sample size = 808), case studies (n = 4), reports of general information about AMD (n = 4), retrospective cohort studies (n = 3), secondary analyses (n = 2), and retrospective case control (n = 1).
How is the impact of AMD measured?
Twenty-five measures were used to describe the impact of vision loss caused by AMD; most studies used more than one. The most frequently used measure was the National Eye Institute Visual Functioning Questionnaire (Mangione et al., 1998), which was used in 23 of the 105 studies. Other frequently used measures were the Short Form Health Surveys (SF-36 or SF-12; n = 10), which emerged from the Medical Outcomes Study (Ware & Sherbourne, 1992). Additional measures included financial cost analyses (n = 9), measures of physical health (n = 8), and time tradeoff (TTO) utility measurement (n = 7).
Are the outcomes reported as solely negative?
Of the 105 reviewed articles, 100 reported negative outcomes, either in full or in part (95 articles reported exclusively negative outcomes, while 5 included mixed findings). None of the articles reported exclusively positive outcomes of vision loss, but five could not be classified as negative due to inconclusive statistical evidence. Representative examples from studies reporting negative findings include the following:
- AMD is a major public health problem with a devastating effect on patients and marked adverse economic consequences for society (Brown et al., 2016).
- We have grossly underestimated the negative impact of AMD, including on our gross domestic product (Gupta, Brown, & Brown, 2007).
- AMD could be a catalyst for great emotional distress (Chung et al., 2015).
- There is an ongoing negative impact of depression caused by AMD (Casten & Rovner, 2013).
Examples of studies in which findings were mixed include one by Ord, Wright, DeAngelis, and Feehan (2015), in which participants identified driving cessation and transportation issues as being important quality-of-life detractors but also emphasized that, despite having AMD, they were committed to engage in and enjoy life. Burton, Shaw, and Gibson (2015) aimed to capture a comprehensive view (negative and positive aspects) of living with AMD and reported both negative and positive outcomes, including increased feelings of kinship, community, self-reliance, and interdependence. The authors cautioned against a blanket attribution of negative connotations to age-related change (in this case, visual acuity) because a negative approach perpetuates the deficit model of aging and prevents us from exploring possibilities for positive change.
Some studies (n = 15) produced inconclusive findings. These studies were looking for negative outcomes but identified either weak or no associations between AMD and a negative outcome. Examples include Klein, Klein, and Knudtson (2005), who investigated frailty among those with AMD, and McGwin et al. (2013), who investigated the association between AMD and motor vehicle crashes but found no association.
Is there evidence that the study design or reported outcomes reinforced the hierarchy of sight?
Of the 105 studies, 102 reinforced the concept of the hierarchy of sight, either by their report of findings or by their design. For example, research participants in some studies were stratified by visual acuity, and findings presented indicated that the lower the acuity, the worse the outcome. The studies that reported exclusively negative outcomes of blindness could only be classified as reinforcing the hierarchy-of-sight concept.
Discussion
We identified a broad and varied body of literature that primarily described as negative the impact that AMD had on individuals, families, and communities. Many approaches have been taken to measure this impact, including qualitative investigations, measuring quality of life and health-related quality of life, estimation of financial impact, TTO scores, and correlations and associations of AMD with negative health care outcomes. The tools used to measure the impact of blindness seem to be inclined toward measuring loss, disability, and lowered expectations of persons diagnosed with AMD.
As hypothesized, there was a preponderance of reporting negative outcomes. According to Rosenthal’s expectancy effect (Rosenthal, 1994; Rosenthal & Jacobson, 1968; Rosenthal & Rubin, 1978), these findings may reflect the social and cultural beliefs that researchers consciously or unconsciously hold about blindness and can become a self-fulfilling prophecy for those with AMD. Our purpose in quantifying this was not to claim that there are not negative outcomes subsequent to vision loss caused by AMD. Rather, our efforts were intended to caution that negative expectations and attitudes reflected in research questions and the outcomes reported may contribute to negative outcomes.
The study design most frequently used to measure the impact of AMD was cross-sectional. Cross-sectional studies can report only associations, not cause and effect. Although the measures were purportedly AMD-specific, it may be that the negative outcomes found in those patients existed separately from the AMD. This latter point might be at least partially understood within the context of the hierarchy of sight (Omvig, 2005).
The term hierarchy of sight was used by Omvig (2002) to describe the assumption that the more sight one has, the better off one will be (Omvig, 2005). We found that, on the surface, this assumption appeared to be supported, as there are many reports of negative outcomes in which the research participants were stratified by acuity, and negative outcomes and visual acuity were significantly correlated. This gives the impression that the degree to which a visually impaired person can succeed and have a full and happy life is governed by the amount of vision he or she has. It also implies that the amount of success a visually impaired person can experience can never be the same as someone who has 20/20 vision. In other words, as visual acuity decreases, so do the possibilities for positive outcomes.
However, other explanations for negative outcomes have been posed. For example, Banerjee, Kumar, Kulhara, and Gupta (2008) reported that negative outcomes assumed to be caused by vision loss were more likely the result of differences in personality. Many factors mediate the relationship of visual acuity to ability and quality of life. For example, Banerjee et al. (2008) reported that general disability was predicted more accurately by depression than by visual acuity. This echoes findings by Brody et al. (2002), who conducted a randomized controlled trial to measure the impact of self-management training designed specifically to meet the needs of individuals with AMD. At the 6-month follow-up, participants in the self-management program reported significantly less emotional distress (p = .008), better function (p = .05), increased self-efficacy (p = .006), and lower clinical depression (p = .05) than the controls. The program was not reversing blindness but was removing barriers in the sociocultural and physical environments. One could surmise that visual acuity was less relevant to positive outcomes than was access to rehabilitative training.
Although there is clear evidence that rehabilitative training reduces depression among the blind and increases and preserves function (Lamoureux et al., 2004; Lamoureux et al., 2007; Teitelman & Copolillo, 2005), there are barriers to older adults accessing this life-changing education. Kaldenberg (2019), in her study of barriers to and facilitators of older adults’ access to low-vision rehabilitative training, cited lack of knowledge of individuals themselves as the number one barrier to this training (90% of individuals with no training were unaware that this training was available); lack of knowledge among medical providers was a close second (73% were unaware of this type of training). Twenty-seven percent of individuals cited lack of transportation as a barrier to training and 53% cited lack of care coordination by their medical provider as a barrier.
Conversely, facilitators of access to this training were (a) the awareness of people around the visually impaired older adult who were aware of the training (including medical providers, friends, and family; 90%) and (b) peer support groups (67%). Transportation assistance facilitated training for 30% of participants (Kaldenberg, 2019).
The scope of research should be broadened to capture not just what is going wrong, but also what is going right, as in the studies by Ord et al. (2015) who reported resilience, and Burton et al. (2015) who identified and reported posttraumatic growth (PTG). PTG describes not just a return to baseline after a traumatic event, as resilience implies, but growth and benefit beyond what an individual experienced before the loss or trauma. Although PTG among individuals experiencing blindness or vision loss has not been studied formally, it is a well-documented process among individuals with many other highly challenging circumstances (Tomich & Helgeson, 2004) and, as such, warrants empirical investigation among visually impaired populations—especially those with AMD. Although vision loss is not desirable, a sole focus on its negative impact on those so affected is potentially counterproductive to a fuller understanding of blindness adjustment and how to best facilitate it.
Limitations
We limited articles by language for practical reasons; relevant articles may have been missed. The study would have been strengthened by including not one, but two reviewers in the first stage of title and abstract screening. Due to the broad search focus and the extremely large number of citations, the resources of this project rendered a second screener for this stage impractical.
Future Directions
A loss-focused paradigm may be clinically disadvantageous for individuals with AMD because what care providers believe and expect can become reality for their patients (Learman et al., 1990; Rosenthal, 1994). In contrast to this negative paradigm, Burton et al. (2015) identified positive outcomes resulting from the struggle with vision loss caused by AMD, including kinship, self-reliance, a strengthened sense of community, and interdependence. There are also anecdotal reports of blindness as a catalyst for positive outcomes.
A significant challenge in the field of blindness and vision loss is to better understand why some individuals thrive while others do not. By expanding research programs to include the discovery of positive outcomes, such as PTG, a more expansive view of the reality of living with vision loss may be achieved, and the pathways to growth and thriving may be better understood and facilitated. A research focus on such positive outcomes might elevate expectations of the psychological and social potential of individuals with AMD. By recognizing patients’ potential for positive outcomes, researchers and providers working with patients with AMD may facilitate them (Calhoun & Tedeschi, 2006). In other words, by considering growth as a potential result of vision loss caused by AMD and addressing this through research and care (when appropriate), positive outcomes may be more easily achieved. Rosenthal’s expectancy effect stands as a caution but also an example; as negative expectations can become self-fulfilling prophecies, so, too, can positive expectations.
Of critical importance is an emphasis toward care planning for older adults with vision loss that includes low-vision rehabilitation and blindness training. Education for both consumers and providers is key, along with ensuring access to transportation in order to access training.
References
References marked with an asterisk indicate articles included solely in the scoping review
*Adachi, K., Wang, E. C. Y., Kudo, K., Crawford, B., Fujita, K., Nagai, Y., . . . Yuzawa, M. (2013). Patient burden associated with wet age-related macular degeneration in Japan. Value in Health, 16(3), A179. doi:10.1016/j.jval.2013.03.897
*Alexander, M. S., Lajoie, K., Neima, D. R., Strath, R. A., Robinovitch, S. N., & Marigold, D. S. (2014). Effects of age-related macular degeneration and ambient light on curb negotiation. Optometry and Vision Science, 91, 975–989. doi: 10.1097/opx.0000000000000286
*Anastasopoulos, E., Yu, F., & Coleman, A. L. (2006). Age-related macular degeneration is associated with an increased risk of hip fractures in the Medicare database. American Journal of Ophthalmology, 142(6), 1081–1083. doi: 10.1016/j.ajo.2006.06.058
Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. doi: 10.1080/1364557032000119616
*Augustin, A., Sahel, J. A., Bandello, F., Dardennes, R., Maurel, F., Negrini, C., Berdeaux, G. (2007). Anxiety and depression prevalence rates in age-related macular degeneration. Investigative Ophthalmology and Visual Science, 48(4), 1498–1503. doi: 10.1167/iovs.06-0761
*Backman, H., & Williams, R. (2002). Living with age-related macular degeneration. Journal of Visual Impairment & Blindness, 96(5), 345–348.
Banerjee, A., Kumar, S., Kulhara, P., & Gupta, A. (2008). Prevalence of depression and its effect on disability in patients with age-related macular degeneration. Indian Journal of Ophthalmology (Poona City), 56(6), 469–474.
Bennion, A. E., Shaw, R. L., & Gibson, J. M. (2012). What do we know about the experience of age related macular degeneration? A systematic review and meta-synthesis of qualitative research. Social Science and Medicine, 75(6), 976–985. doi: 10.1016/j.socscimed.2012.04.023
*Berdeaux, G. H., Nordmann, J. P., Colin, E., & Arnould, B. (2005). Vision-related quality of life in patients suffering from age-related macular degeneration. American Journal of Ophthalmology, 139(2), 271–279. doi: 10.1016/j.ajo.2004.09.028
*Berman, K., & Brodaty, H. (2006). Psychosocial effects of age-related macular degeneration. International Psychogeriatrics, 18(3), 415–428. doi: 10.1017/s1041610205002905
*Boland, M. R. S., Vingerling, J., Groot, M., & Hakkaart-van Roijen, L. (2011). PSS9 the burden of age-related macular degeneration in the Netherlands. Value in Health, 14(7), A503. doi: 10.1016/j.jval.2011.08.1474
*Bonastre, J., Le Pen, C., Anderson, P., Ganz, A., Berto, P., & Berdeaux, G. (2002). The epidemiology, economics and quality of life burden of age-related macular degeneration in France, Germany, Italy and the United Kingdom. The European Journal of Health Economics, 3(2), 94–102. doi: 10.1007/s10198-002-0104-y
*Bonastre, J., Le Pen, C., Soubrane, G., & Quentel, G. (2003). The burden of age-related macular degeneration: Results of a cohort study in two French referral centres. Pharmacoeconomics, 21(3), 181–190.
*Brennan, M., Horowitz, A., Reinhardt, J. P., Stuen, C., Rubio, R., & Oestreicher, N. (2011). The societal impact of age-related macular degeneration: Use of social support resources differs by the severity of the impairment. Journal of Visual Impairment & Blindness, 105(1), 5–19.
*Brody, B. L., Field, L. C., Roch-Levecq, A. C., Depp, C., Edland, S. D., Minasyan, L., & Brown, S. I. (2012). Computer use among patients with age-related macular degeneration. Ophthalmic Epidemiology, 19(4), 190–195. doi: 10.3109/09286586.2012.672618
*Brody, B. L., Gamst, A. C., Williams, R. A., Smith, A. R., Lau, P. W., Dolnak, D., . . . Brown, S. I. (2001). Depression, visual acuity, comorbidity, and disability associated with age-related macular degeneration. Ophthalmology, 108(10), 1893–1900; discussion 1900–1901.
Brody, B. L., Roch-Levecq, A., Gamst, A. C., Maclean, K., Kaplan, R. M., & Brown, S. I. (2002). Self-management of age-related macular degeneration and quality of life: A randomized controlled trial. Archives of Ophthalmology, 120(11), 1477–1483. doi: 10.1001/archopht.120.11.1477
*Brown, G. C., Brown, M. M., Sharma, S., Stein, J. D., Roth, Z., Campanella, J., & Beauchamp, G. R. (2005). The burden of age-related macular degeneration: A value-based medicine analysis. Transactions of the American Ophthalmological Society, 103, 173–186.
*Brown, G. C., Sharma, S., Brown, M. M., & Kistler, J. (2000). Utility values and age-related macular degeneration. Archives of Ophthalmology, 118(1), 47–51.
Brown, M. M., Brown, G. C., Lieske, H. B., Tran, I., Turpcu, A., & Colman, S. (2016). Societal costs associated with neovascular age-related macular degeneration in the United States. Retina, 36(2), 285–298. doi: 10.1097/iae.0000000000000717
*Brown, M. M., Brown, G. C., Sharma, S., Landy, J., & Bakal, J. (2002). Quality of life with visual acuity loss from diabetic retinopathy and age-related macular degeneration. Archives of Ophthalmology, 120(4), 481–484.
*Brown, M. M., Brown, G. C., Stein, J. D., Roth, Z., Campanella, J., & Beauchamp, G. R. (2005). Age-related macular degeneration: Economic burden and value-based medicine analysis. Canadian Journal of Ophthalmology, 40(3), 277–287. doi: 10.1016/s0008-4182(05)80070-5
Burton, A. E., Shaw, R. L., & Gibson, J. M. (2015). Living together with age-related macular degeneration: An interpretative phenomenological analysis of sense-making within a dyadic relationship. Journal of Health Psychology, 20(10), 1285–1295. doi: 10.1177/1359105313511134
*Buss, D. D. (1993). Storm of the eye. Macular degeneration: The forgotten plague. Contemporary Long-term Care, 16(11), 62–63, 65–67.
*Cahill, M. T., Banks, A. D., Stinnett, S. S., & Toth, C. A. (2005). Vision-related quality of life in patients with bilateral severe age-related macular degeneration. Ophthalmology, 112(1), 152–158. doi: 10.1016/j.ophtha.2004.06.036
Calhoun, L. G., & Tedeschi, R. G. (2006). Handbook of post-traumatic growth: Research and practice. Mahwah, NJ: Erlbaum.
*Casey, D. A., & Wandzilak, T. (1988). Senile macular degeneration and psychosis. Journal of Geriatric Psychiatry and Neurology, 1(2), 108–109.
*Casten, R. J., & Rovner, B. (2008). Depression in age-related macular degeneration. Journal of Visual Impairment & Blindness, 102(10), 591–599.
Casten, R. J., & Rovner, B. W. (2013). Update on depression and age-related macular degeneration. Current Opinion in Ophthalmology, 24(3), 239–243. doi: 10.1097/ICU.0b013e32835f8e55
*Casten, R. J., Rovner, B. W., & Edmonds, S. E. (2002). The impact of depression in older adults with age-related macular degeneration. Journal of Visual Impairment & Blindness, 96(6), 399–406.
*Casten, R. J., Rovner, B. W., & Tasman, W. (2004). Age-related macular degeneration and depression: A review of recent research. Current Opinion in Ophthalmology, 15(3), 181–183.
*Chakravarthy, U., & Stevenson, M. (2005). Self-reported visual functioning and quality of life in age-related macular degeneration. Current Opinion in Ophthalmology, 16(3), 179–183.
Chan, N. Y.-G., Fujiyama, T., & Rubin, G. S. (2015). Investigating the relationship between public transport difficulty and life-space for people with age related macular degeneration and glaucoma. Investigative Ophthalmology and Visual Science, 56, 501–501.
*Chatziralli, I., Mitropoulos, P., Parikakis, E., Niakas, D., & Labiris, G. (2017). Risk factors for poor quality of life among patients with age-related macular degeneration. Seminars in Ophthalmology, 32(6), 772–780. doi: 10.1080/08820538.2016.1181192
*Cho, H., Lee, W., & Sobrin, L. (2014). Risk factors for depressive symptoms in age-related macular degeneration based on the fifth (2011) Korea national health and nutrition examination survey (knhanes v-2). Investigative Ophthalmology and Visual Science, 55(13), 668–668.
*Choudhury, F., Varma, R., Klein, R., Gauderman, W. J., Azen, S. P., & McKean-Cowdin, R. (2016). Age-related macular degeneration and quality of life in Latinos: The Los Angeles Latino Eye Study. JAMA Ophthalmology, 134(6), 683–690. doi: 10.1001/jamaophthalmol.2016.0794
Chung, S.-D., Ho, J.-D., Hwa, P., Lee, H.-C., & Lin, H.-C. (2015). Increased risk of depressive disorder following a diagnosis of neovascular age-related macular degeneration. Acta Ophthalmologica, 93(2), e176–e177. doi: 10.1111/aos.12478
Chung, S.-D., Hu, C.-C., Lin, H.-C., Kao, L.-T., & Huang, C.-C. (2017). Increased fall risk in patients with neovascular age-related macular degeneration: A three-year follow-up study. Acta Ophthalmologica, 95(8), e800–e801. doi: 10.1111/aos.13281
*Cimarolli, V. R., Boerner, K., Brennan-Ing, M., Reinhardt, J. P., & Horowitz, A. (2012). Challenges faced by older adults with vision loss: A qualitative study with implications for rehabilitation. Clinical Rehabilitation, 26(8), 748–757. doi: 10.1177/0269215511429162
*Cimarolli, V. R., Casten, R. J., Rovner, B. W., Heyl, V., Sörensen, S., & Horowitz, A. (2015). Anxiety and depression in patients with advanced macular degeneration: Current perspectives. Clinical Ophthalmology (Auckland, N.Z.), 10, 55–63. doi: 10.2147/OPTH.S80489
Conrad, P., Mackie, T., & Mehrotra, A. (2010). Estimating the costs of medicalization. Social Science & Medicine, 70(12), 1943–1947. doi: 10.1016/j.socscimed.2010.02.019
*Cruess, A., Zlateva, G., Xu, X., & Rochon, S. (2007). Burden of illness of neovascular age-related macular degeneration in Canada. Canadian Journal of Ophthalmology, 42(6), 836–843. doi: 10.3129/i07-153
*Cruess, A., Zlateva, G., Xu, X., Soubrane, G., Pauleikhoff, D., Lotery, A., . . . Goss, T. F. (2008). Economic burden of bilateral neovascular age-related macular degeneration: Multi-country observational study. Pharmacoeconomics, 26(1), 57–73.
*Dahlin-Ivanoff, S., Sjöstrand, J., Klepp, K. I., Lind, L. A., & Lindqvist, B. L. (1996). Planning a health education programme for the elderly visually impaired person—A focus group study. Disability and Rehabilitation, 18(10), 515–522. doi: 10.3109/09638289609166038
*Dahlin-Ivanoff, S., Sonn, U., Lundgren-Lindqvist, B., Sjöstrand, J., & Steen, B. (2000). Disability in daily life activities and visual impairment: A population study of 85-year-old people living at home. Scandinavian Journal of Occupational Therapy, 7(4), 148–155. doi: 10.1080/110381200300008689
*Dawson, S. R., Mallen, C. D., Gouldstone, M. B., Yarham, R., & Mansell, G. (2014). The prevalence of anxiety and depression in people with age-related macular degeneration: A systematic review of observational study data. BMC Ophthalmology, 14, 78. doi: 10.1186/1471-2415-14-78
*DeCarlo, D. K., Scilley, K., Wells, J., & Owsley, C. (2003). Driving habits and health-related quality of life in patients with age-related maculopathy. Optometry and Vision Science, 80(3), 207–213.
*Dilokthornsakul, P., Chaiyakunapruk, N., Ruamviboonsuk, P., Ratanasukon, M., Ausayakhun, S., Tungsomeroengwong, A., . . . Chanatittarat, C. (2014). Health resource utilization and the economic burden of patients with wet age-related macular degeneration in Thailand. International Journal of Ophthalmology, 7(1), 145–151. doi: 10.3980/j.issn.2222-3959.2014.01.27
*Elshout, M., van der Reis, M. I., de Jong-Hesse, Y., Webers, C. A., & Schouten, J. S. (2016). Distinguishing between better and worse visual acuity by studying the correlation with quality of life in neovascular age-related macular degeneration. Ophthalmology, 123(11), 2408–2412. doi: 10.1016/j.ophtha.2016.07.015
*Elshout, M., Webers, C. A., van der Reis, M. I., de Jong-Hesse, Y., & Schouten, J. S. (2017). Tracing the natural course of visual acuity and quality of life in neovascular age-related macular degeneration: A systematic review and quality of life study. BMC Ophthalmology, 17(1), 120. doi: 10.1186/s12886-017-0514-3
*Fenwick, E. K., Cheung, C. M. G., Ong, P. G., Tan, G., Lee, S. Y., Yeo, I., . . . Lamoureux, E. L. (2017). The impact of typical neovascular age-related macular degeneration and polypoidal choroidal vasculopathy on vision-related quality of life in Asian patients. British Journal of Ophthalmology, 101(5), 591–596. doi: 10.1136/bjophthalmol-2016-308541
*Ferris, F. L. I. (2005). Vision-related quality of life in patients suffering from age-related macular degeneration. Evidence-Based Ophthalmology, 6(3), 163–164. doi: 10.1097/01.ieb.0000169322.72430.82
*Girdler, S., Packer, T. L., & Boldy, D. (2008). The impact of age-related vision loss. OTJR: Occupation, Participation and Health, 28(3), 110–120. doi: 10.3928/15394492-20080601-05
*Gopinath, B., Kifley, A., Cummins, R., Heraghty, J., & Mitchell, P. (2015). Predictors of psychological distress in caregivers of older persons with wet age-related macular degeneration. Aging and Mental Health, 19(3), 239–246. doi: 10.1080/13607863.2014.924477
*Gopinath, B., Liew, G., Burlutsky, G., & Mitchell, P. (2014). Age-related macular degeneration and 5-year incidence of impaired activities of daily living. Maturitas, 77(3), 263–266. doi: 10.1016/j.maturitas.2013.12.001
Gupta, O. P., Brown, G. C., & Brown, M. M. (2007). Age-related macular degeneration: The costs to society and the patient. Current Opinion in Ophthalmology, 18(3), 201–205. doi: 10.1097/ICU.0b013e32810c8df4
*Hassan, S. E., Lovie-Kitchin, J. E., & Woods, R. L. (2002). Vision and mobility performance of subjects with age-related macular degeneration. Optometry and Vision Science, 79(11), 697–707.
*Hassell, J. B., Lamoureux, E. L., & Keeffe, J. E. (2006). Impact of age related macular degeneration on quality of life. British Journal of Ophthalmology, 90(5), 593–596. doi: 10.1136/bjo.2005.086595
Ivers, R. Q., Cumming, R. G., Mitchell, P., Simpson, J. M., & Peduto, A. J. (2003). Visual risk factors for hip fracture in older people. Journal of the American Geriatrics Society, 51(3), 356–363.
Jager, R. D., Mieler, W. F., & Miller, J. W. (2008). Age-related macular degeneration. The New England Journal of Medicine, 358(24), 2606–2617. doi: 10.1056/NEJMra0801537
Jernigan, K. (1984). Blindness: The circle of sophistry. Retrieved from www.blind.net/a-philosophy-of-blindness/banq-add/banqadd-1984.html
*Jivraj, J., Jivraj, I., Tennant, M., & Rudnisky, C. (2013). Prevalence and impact of depressive symptoms in patients with age-related macular degeneration. Canadian Journal of Ophthalmology, 48(4), 269–273. doi: 10.1016/j.jcjo.2013.03.007
Joyce, K. (2008). Magnetic appeal: MRI and the myth of transparency. Ithaca, NY: Cornell University Press.
Kaldenberg, J. (2019). Low vision rehabilitation services: Perceived barriers and facilitators to access for older adults with visual impairment. British Journal of Occupational Therapy, 82(8), 466–474.
Klein, R., Klein, B. E., & Knudtson, M. D. (2005). Frailty and age-related macular degeneration: The Beaver Dam Eye Study. American Journal of Ophthalmology, 140(1), 129–131. doi: 10.1016/j.ajo.2004.12.049
Kuyk, T., Liu, L., Elliott, J. L., Grubbs, H. E., Owsley, C., McGwin, G., Jr., . . . Fuhr, P. S. (2008). Health-related quality of life following blind rehabilitation. Quality of Life Research, 17(4), 497–507. doi: 10.1007/s11136-008-9336-3
Lamoureux, E. L., Hassell, J. B., & Keeffe, J. E. (2004). The determinants of participation in activities of daily living in people with impaired vision. American Journal of Ophthalmology, 137(2), 265–270. doi: 10.1016/j.ajo.2003.08.003
*Lamoureux, E. L., Mitchell, P., Rees, G., Cheung, G., Yeo, I., Lee, S. Y., . . . Wong, T. Y. (2011). Impact of early and late age-related macular degeneration on vision-specific functioning. British Journal of Ophthalmology, 95(5), 666–670. doi: 10.1136/bjo.2010.185207
Lamoureux, E. L., Pallant, J. F., Pesudovs, K., Rees, G., Hassell, J. B., & Keeffe, J. E. (2007). The effectiveness of low-vision rehabilitation on participation in daily living and quality of life. Investigative Ophthalmology & Visual Science, 48(4), 1476–1482.
Learman, L. A., Avorn, J., Everitt, D. E., & Rosenthal, R. (1990). Pygmalion in the nursing home: The effects of caregiver expectations on patient outcomes. Journal of the American Geriatrics Society, 38(7), 797–803.
*Lee, W. J., Cho, H. Y., Kim, D. H., Yu, H. G., Oh, J., Kim, J. S., & Moon, S. W. (2013). Depression of late age-related macular degeneration patients in Korea. The Asia-Pacific Journal of Ophthalmology, 2(1), 23–27. doi: 10.1097/APO.0b013e31827be8b1
Levac, D., Colquhoun, H., & O’Brien, K. K. (2010). Scoping studies: Advancing the methodology. Implementation Science, 5, Article 69. doi: 10.1186/1748-5908-5-69
*Lopez-Miguel, A., Coco-Martin, M. B., Martinez-Fernandez, R., Gomez-Ramirez, A. M., Garcia-Ayuso, D., Sobrado-Calvo, P., & Maldonado, M. J. (2013). Patient-reported outcomes in Spanish patients diagnosed with bilateral age-related macular degeneration. International Journal of Ophthalmology, 230(2), 69–75. doi: 10.1159/000351652
*Loprinzi, P. D., Swenor, B. K., & Ramulu, P. Y. (2015). Age-related macular degeneration is associated with less physical activity among us adults: Cross-sectional study. PLoS One, 10(5), e0125394. doi: 10.1371/journal.pone.0125394
*Lotery, A., Xu, X., Zlatava, G., & Loftus, J. (2007). Burden of illness, visual impairment and health resource utilisation of patients with neovascular age-related macular degeneration: Results from the UK cohort of a five-country cross-sectional study. British Journal of Ophthalmology, 91(10), 1303–1307. doi: 10.1136/bjo.2007.116939
*Mangione, C. M., Gutierrez, P. R., Lowe, G., Orav, E. J., & Seddon, J. M. (1999). Influence of age-related maculopathy on visual functioning and health-related quality of life. American Journal of Ophthalmology, 128(1), 45–53.
Mangione, C. M., Lee, P. P., Pitts, J., Gutierrez, P., Berry, S., & Hays, R. D. (1998). Psychometric properties of the National Eye Institute Visual Function Questionnaire (NEI-VFQ). NEI-VFQ field test investigators. Archives of Ophthalmology, 116(11), 1496–1504.
Marback, R. F., Maia, O. O., Jr., Morais, F. B., & Takahashi, W. Y. (2007). Quality of life in patients with age-related macular degeneration with monocular and binocular legal blindness. Clinics (Sao Paulo), 62(5), 573–578.
Mays, N., Roberts, E., & Popay, J. (2001). Synthesising research evidence. In N. Fulop, P. Allen, A. Clarke, & N. Black (Eds.), Studying the organisation and delivery of health services: Research methods (pp. 188–220). London, United Kingdom: Routledge.
McGwin, G., Jr., Mitchell, B., Searcey, K., Albert, M. A., Feist, R., Mason, J. O., 3rd, . . . Owsley, C. (2013). Examining the association between age-related macular degeneration and motor vehicle collision involvement: A retrospective cohort study. British Journal of Ophthalmology, 97(9), 1173–1176. doi: 10.1136/bjophthalmol-2013-303601
Meyer-Ruesenberg, B., & Richard, G. (2010). New insights into the underestimated impairment of quality of life in age-related macular degeneration—A review of the literature. Klinische Monatsblatter für Augenheilkunde, 227(8), 646–652. doi: 10.1055/s-0029-1245118
*Mitchell, J., & Bradley, C. (2006). Quality of life in age-related macular degeneration: A review of the literature. Health & Quality of Life Outcomes, 4, 97–97. doi: 10.1186/1477-7525-4-97
Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Medicine, 6(7), e1000097. doi: 10.1371/journal.pmed.1000097
*Moore, L. W., & Miller, M. (2005). Driving strategies used by older adults with macular degeneration: Assessing the risks. Applied Nursing Research, 18(2), 110–116. doi: 10.1016/j.apnr.2004.06.014
National Eye Institute. (n.d.). Prevalence of age-related macular degeneration. Retrieved from https://nei.nih.gov/eyedata/pbd4
Omvig, J. H. (2002). Freedom for the blind. Fayetteville, AR: University of Arkansas.
Omvig, J.H. (2004, July). Great expectations: From the hierarchy of sight to the hierarchy of truth. Braille Monitor, 47(7). Retrieved from https://archive.nfb.org/images/nfb/publications/bm/bm04/bm0407/bm040702.htm
Omvig, J. H. (2005). The blindness revolution: Jernigan in his own words. Greenwich, CT: Information Age.
Ord, L. M., Wright, J., DeAngelis, M. M., & Feehan, M. (2015). Quality of life with macular degeneration is not as dark as it may seem: Patients’ perceptions of the MacDQoL questionnaire. Journal of Clinical Medicine, 4(9), 1841–1852. doi: 10.3390/jcm4091841
*Orticio, L. P. (2011). The impact of vision loss from age-related macular degeneration: A review (part 1). Insight, 36(4), 13–15.
*Owsley, C., Huisingh, C., Clark, M. E., Jackson, G. R., & McGwin, G., Jr. (2016). Comparison of visual function in older eyes in the earliest stages of age-related macular degeneration to those in normal macular health. Current Eye Research, 41(2), 266–272. doi: 10.3109/02713683.2015.1011282
Owsley, C., & McGwin, G., Jr. (2008). Driving and age-related macular degeneration. Journal of Visual Impairment & Blindness, 102(10), 621–635.
*Owsley, C., & McGwin, G., Jr. (2016). Vision-targeted health related quality of life in older adults: Patient-reported visibility problems in low luminance activities are more likely to decline than daytime activities. BMC Ophthalmology, 16, 92. doi: 10.1186/s12886-016-0274-5
*Pardhan, S., Gonzalez-Alvarez, C., & Subramanian, A. (2011). How does the presence and duration of central visual impairment affect reaching and grasping movements? Ophthalmic and Physiological Optics, 31(3), 233–239. doi: 10.1111/j.1475-1313.2010.00819.x
*Pardhan, S., & Zuidhoek, S. (2013). Dual cognitive task affects reaching and grasping behavior in subjects with macular disorders. Investigative Ophthalmology and Visual Science, 54(5), 3281–3288. doi: 10.1167/iovs.12-11045
*Paulus, Y. M., Jefferys, J. L., Hawkins, B. S., & Scott, A. W. (2017). Visual function quality of life measure changes upon conversion to neovascular age-related macular degeneration in second eyes. Quality of Life Research, 26(8), 2139–2151. doi: 10.1007/s11136-017-1547-z
Pham, M. T., Rajic, A., Greig, J. D., Sargeant, J. M., Papadopoulos, A., & McEwen, S. A. (2014). A scoping review of scoping reviews: Advancing the approach and enhancing the consistency. Research Synthesis Methods, 5(4), 371–385. doi: 10.1002/jrsm.1123
Rein, D. B., Wittenborn, J. S., Zhang, X., Honeycutt, A. A., Lesesne, S. B., & Saaddine, J. (2009). Forecasting age-related macular degeneration through the year 2050: The potential impact of new treatments. Archives of Ophthalmology, 127(4), 533–540. doi: 10.1001/archophthalmol.2009.58
Rosenthal, R. (1994). Interpersonal expectancy effects: A 30-year perspective. Current Directions in Psychological Science, 3(6), 176–179. doi: 10.1111/1467-8721.ep10770698
Rosenthal, R., & Jacobson, L. (1966). Teachers’ expectancies: Determinants of pupils’ IQ gains. Psychological Reports, 19(1), 115–118. doi: 10.2466/pr0.1966.19.1.115
Rosenthal, R., & Jacobson, L. (1968). Pygmalion in the classroom: Teacher expectation and pupils’ intellectual development. New York, NY: Holt, Rinehart & Winston.
Rosenthal, R., & Rubin, D. (1978). Interpersonal expectancy effect: The first 345 studies. Behavioral and Brain Sciences, 1(3), 377–386.
*Rovner, B. W., & Casten, R. J. (2002). Activity loss and depression in age-related macular degeneration. American Journal of Geriatric Psychiatry, 10(3), 305–310.
*Rovner, B. W., Casten, R. J., Hegel, M. T., & Tasman, W. S. (2006). Minimal depression and vision function in age-related macular degeneration. Ophthalmology, 113(10), 1743–1747. doi: 10.1016/j.ophtha.2006.05.033
*Sahel, J. A., Bandello, F., Augustin, A., Maurel, F., Negrini, C., & Berdeaux, G. H. (2007). Health-related quality of life and utility in patients with age-related macular degeneration. Archives of Ophthalmology, 125(7), 945–951. doi: 10.1001/archopht.125.7.945
*Schmier, J. K., Halpern, M. T., Covert, D., Delgado, J., & Sharma, S. (2006). Impact of visual impairment on use of caregiving by individuals with age-related macular degeneration. Retina, 26(9), 1056–1062. doi: 10.1097/01.iae.0000254890.48272.5a
*Schmier, J. K., Jones, M. L., & Halpern, M. T. (2006). The burden of age-related macular degeneration. Pharmacoeconomics, 24(4), 319–334.
*Scilley, K., DeCarlo, D. K., Wells, J., & Owsley, C. (2004). Vision-specific health-related quality of life in age-related maculopathy patients presenting for low vision services. Ophthalmic Epidemiology, 11(2), 131–146.
*Scilley, K., Jackson, G. R., Cideciyan, A. V., Maguire, M. G., Jacobson, S. G., & Owsley, C. (2002). Early age-related maculopathy and self-reported visual difficulty in daily life. Ophthalmology, 109(7), 1235–1242.
*Scott, I. U., Feuer, W. J., & Jacko, J. A. (2002). Impact of visual function on computer task accuracy and reaction time in a cohort of patients with age-related macular degeneration. American Journal of Ophthalmology, 133(3), 350–357.
*Sengupta, S., Nguyen, A. M., van Landingham, S. W., Solomon, S. D., Do, D. V., Ferrucci, L., . . . Ramulu, P. Y. (2015). Evaluation of real-world mobility in age-related macular degeneration. BMC Ophthalmology, 15, 9. doi: 10.1186/1471-2415-15-9
*Sengupta, S., van Landingham, S. W., Solomon, S. D., Do, D. V., Friedman, D. S., & Ramulu, P. Y. (2014). Driving habits in older patients with central vision loss. Ophthalmology, 121(3), 727–732. doi: 10.1016/j.ophtha.2013.09.042
*Slakter, J. S., & Stur, M. (2005). Quality of life in patients with age-related macular degeneration: Impact of the condition and benefits of treatment. Survey of Ophthalmology, 50(3), 263–273. doi: 10.1016/j.survophthal.2005.02.007
*Stein, J. D., Brown, M. M., Brown, G. C., Hollands, H., & Sharma, S. (2003). Quality of life with macular degeneration: Perceptions of patients, clinicians, and community members. British Journal of Ophthalmology, 87(1), 8–12.
*Stevenson, M. R., Hart, P. M., Montgomery, A. M., McCulloch, D. W., & Chakravarthy, U. (2004). Reduced vision in older adults with age related macular degeneration interferes with ability to care for self and impairs role as carer. British Journal of Ophthalmology, 88(9), 1125–1130. doi: 10.1136/bjo.2003.032383
*Subhi, Y., & Sorensen, T. L. (2016). Physical activity patterns in patients with early and late age-related macular degeneration. Danish Medical Journal, 63(11), 1–5.
*Sun, C., Tikellis, G., Klein, R., Steffens, D. C., Larsen, E. K., & Wong, T. Y. (2007). Depressive symptoms and age-related macular degeneration in older people: The cardiovascular health study. Ophthalmic Epidemiology, 14(3), 127–133. doi: 10.1080/09286580601186742
*Swagerty, D. L., Jr. (1995). The impact of age-related visual impairment on functional independence in the elderly. Kansas Medicine, 96(1), 24–26.
*Szabo, S. M., Janssen, P. A., Khan, K., Potter, M. J., & Lord, S. R. (2008). Older women with age-related macular degeneration have a greater risk of falls: A physiological profile assessment study. Journal of the American Geriatrics Society, 56(5), 800–807. doi: 10.1111/j.1532-5415.2008.01666.x
*Szlyk, J. P., Pizzimenti, C. E., Fishman, G. A., Kelsch, R., Wetzel, L. C., Kagan, S., & Ho, K. (1995). A comparison of driving in older subjects with and without age-related macular degeneration. Archives of Ophthalmology, 113(8), 1033–1040.
*Taylor, D. J., Hobby, A. E., Binns, A. M., & Crabb, D. P. (2016). How does age-related macular degeneration affect real-world visual ability and quality of life? A systematic review. BMJ Open, 6(12), e011504. doi: 10.1136/bmjopen-2016-011504
Teitelman, J., & Copolillo, A. (2005). Psychosocial issues in older adults' adjustment to vision loss: Findings from qualitative interviews and focus groups. American Journal of Occupational Therapy, 59(4), 409–417.
Tomich, P. L., & Helgeson, V. S. (2004). Is finding something good in the bad always good? Benefit finding among women with breast cancer. Health Psychology, 23(1), 16–23. doi: 10.1037/0278-6133.23.1.16
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K., Colquhoun, H, Kastner, M., . . . Straus, S. E. (2016). A scoping review on the conduct and reporting of scoping reviews. BMC Medical Research Methodology, 16(1). doi: 10.1186/s12874-016-0116-4
*van de Graaf, E. S., Despriet, D. D. G., Klaver, C. C. W., & Simonsz, H. J. (2016). Patient-reported utilities in bilateral visual impairment from amblyopia and age-related macular degeneration. BMC Ophthalmology, 16(1). doi: 10.1186/s12886-016-0234-0
*van Landingham, S. W., Massof, R. W., Chan, E., Friedman, D. S., & Ramulu, P. Y. (2014). Fear of falling in age-related macular degeneration. BMC Ophthalmology, 14(1). doi: 10.1186/1471-2415-14-10
*Varano, M., Eter, N., Winyard, S., Wittrup-Jensen, K. U., Navarro, R., & Heraghty, J. (2016). The emotional and physical impact of wet age-related macular degeneration: Findings from the WAMD patient and caregiver survey. Clinical Ophthalmology (Auckland, N.Z.), 10(1), 257–267. doi: 10.2147/opth.s92616
Vu, H. T. V., Keeffe, J. E., McCarty, C. A., & Taylor, H. R. (2005). Impact of unilateral and bilateral vision loss on quality of life. British Journal of Ophthalmology, 89(3), 360–363. doi: 10.1136/bjo.2004.047498
Wang, J. J., Mitchell, P., Cumming, R. G., & Smith, W. (2003). Visual impairment and nursing home placement in older Australians: The Blue Mountains Eye Study. Ophthalmic Epidemiology, 10(1), 3–13.
Wang, J. J., Mitchell, P., & Smith, W. (2000). Vision and low self-rated health: The Blue Mountains Eye Study. Investigative Ophthalmology and Visual Science, 41(1), 49–54.
Wang, J. J., Mitchell, P., Smith, W., Cumming, R. G., & Attebo, K. (1999). Impact of visual impairment on use of community support services by elderly persons: The Blue Mountains Eye Study. Investigative Ophthalmology and Visual Science, 40(1), 12–19.
*Wang, M. Y., Rousseau, J., Boisjoly, H., Schmaltz, H., Kergoat, M. J., Moghadaszadeh, S., . . . Freeman, E. E. (2012). Activity limitation due to a fear of falling in older adults with eye disease. Investigative Ophthalmology and Visual Science, 53(13), 7967–7972. doi: 10.1167/iovs.12-10701
*Wang, Y. Z., Wilson, E., Locke, K. G., & Edwards, A. O. (2002). Shape discrimination in age-related macular degeneration. Investigative Ophthalmology and Visual Science, 43(6), 2055–2062.
Ware, J. E., Jr., & Sherbourne, C. D. (1992). The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Medical Care, 30(6), 473–483.
Weih, L. M., Hassell, J. B., & Keeffe, J. (2002). Assessment of the impact of vision impairment. Investigative Ophthalmology and Visual Science, 43(4), 927–935.
West, S. K., Munoz, B., Rubin, G. S., Schein, O. D., Bandeen-Roche, K., Zeger, S., . . . Fried, L. P. (1997). Function and visual impairment in a population-based study of older adults: The See Project. Salisbury eye evaluation. Investigative Ophthalmology and Visual Science, 38(1), 72–82.
West, S. K., Rubin, G. S., Broman, A. T., Munoz, B., Bandeen-Roche, K., & Turano, K. (2002). How does visual impairment affect performance on tasks of everyday life? The SEE Project. Salisbury eye evaluation. Archives of Ophthalmology, 120(6), 774–780.
*Weyer-Wendl, H., & Walter, P. (2016). Financial burden and quality of life of informal caregivers of patients with wet age-related macular degeneration. Health Economics Review, 6(1), 37. doi: 10.1186/s13561-016-0116-4
*Williams, R. A., Brody, B. L., Thomas, R. G., Kaplan, R. M., & Brown, S. I. (1998). The psychosocial impact of macular degeneration. Archives of Ophthalmology, 116(4), 514–520.
*Wood, J. M., Lacherez, P., Black, A. A., Cole, M. H., Boon, M. Y., & Kerr, G. K. (2011). Risk of falls, injurious falls, and other injuries resulting from visual impairment among older adults with age-related macular degeneration. Investigative Ophthalmology and Visual Science, 52(8), 5088–5092. doi: 10.1167/iovs.10-6644
World Health Organization. (n.d.). Priority eye diseases. Retrieved from http://www.who.int/blindness/causes/priority/en/index8.html
*Wysong, A., Lee, P. P., & Sloan, F. A. (2009). Longitudinal incidence of adverse outcomes of age-related macular degeneration. Archives of Ophthalmology, 127(3), 320–327. doi: 10.1001/archophthalmol.2008.613
Table 1
Inclusion and Exclusion Criteria
Criterion |
Inclusion |
Exclusion |
|---|---|---|
Time period |
No dates excluded |
No dates excluded |
Language |
English |
Other than English |
Type of article |
Original research published in peer-reviewed journal, non-study reportspublished in peer-reviewed journal |
Articles not peer reviewed or reporting on original research |
Study focus |
The impact of age-related macular degeneration (AMD) or outcome attributed to AMD |
Pathophysiology, physiology, treatment of retina, pharmacodynamics, photodynamics, value-based medicine (cost-effectiveness of treatment), risk factors for AMD, prediction of AMD, nutrition and AMD, genetics and AMD, anxiety around injections/treatment, randomized controlled trial, adjustment, rehabilitation, quality of life after treatment, quality-of-life/utility instrument assessment |
Literature focus |
Articles in which the overarching theme related to the impact of AMD or outcomes attributed to AMD |
Articles that made a passing or token reference to the impact of AMD |
Population and sample |
Visually impaired older adults, individuals with AMD |
Individuals with a diagnosis other than AMD |
Table 2
Key Features of Included Articles
Element |
n |
% |
|---|---|---|
Publication Years |
|
|
1988–1990 |
1 |
1.0 |
1991–2000 |
9 |
8.6 |
2001–2010 |
48 |
45.7 |
2011 and later |
47 |
44.8 |
Journals |
|
|
Investigative Ophthalmology & Visual Science |
8 |
7.6 |
British Journal of Ophthalmology |
7 |
6.7 |
Archives of Ophthalmology |
6 |
5.7 |
BMC Ophthalmology |
6 |
5.7 |
Ophthalmology |
6 |
5.7 |
American Journal of Ophthalmology |
5 |
4.8 |
Current Opinion in Ophthalmology |
5 |
4.8 |
Journal of Visual Impairment & Blindness |
5 |
4.8 |
Other |
57 |
54.3 |
Types of Studies |
|
|
Cross-sectional |
69 |
65.7 |
Review of literature |
15 |
14.3 |
Longitudinal |
7 |
6.7 |
Case study |
4 |
3.8 |
Report |
4 |
3.8 |
Retrospective cohort |
3 |
2.9 |
Secondary analysis |
2 |
1.9 |
Case control |
1 |
.95 |
Outcome Measures |
|
|
NEI VFQ—any |
23 |
21.9 |
SF—any |
10 |
9.5 |
Cost and resource measures |
9 |
8.6 |
Physical health measures |
8 |
7.6 |
TTO |
6 |
5.7 |
Driving measures |
6 |
5.7 |
Walking, physical activity measures |
6 |
5.7 |
VF—any, other functional vision |
6 |
5.7 |
GDS (& GDS-S-J & GDS-K) |
5 |
4.8 |
Living space measures |
5 |
4.8 |
HADS |
4 |
3.8 |
CES-D |
4 |
3.8 |
DLTV |
4 |
3.8 |
Falling/fractures |
4 |
3.8 |
Other depression measures |
4 |
3.8 |
Other QOL |
4 |
3.8 |
ADVS |
3 |
2.9 |
MacDQoL |
3 |
2.9 |
HRQOL & other health-related QOL or health & impact |
3 |
2.9 |
Other ADL |
3 |
2.9 |
Reach and grasp |
3 |
2.9 |
EQ-5D |
2 |
1.9 |
IVI |
2 |
1.9 |
I-ADL |
2 |
1.9 |
Family and social support |
1 |
1.0 |
Findings Postures |
|
|
Negative |
95 |
90.5 |
Mixed |
5 |
4.8 |
Inconclusive |
5 |
4.8 |
Reinforced Hierarchy of Sight |
|
|
Yes |
102 |
97.14 |
No |
3 |
2.86 |
Sample Size |
M |
IQR |
Cross-sectional studies |
333 |
254 |
Longitudinal studies |
808 |
548 |
Note. N = 105. NEI VFQ-25 = National Eye Institute Visual Function Questionnaire; SF = short form; SF-12 = Medical Outcomes Survey Short Form; SF-36 = Short Form Health Survey; TTO = time tradeoff; VF = visual fields; HADS = Hospital Anxiety and Depression Scale; CES-D = Center for Epidemiological Studies-Depression Scale; DLTV = daily living tasks dependent on vision; QOL = quality of life; ADVS = Activities of Daily Vision Scale; MacDQoL = Macular Degeneration Quality of Life Scale; HRQOL = health-related quality of life; ADL = activities of daily living; EQ-5D = EuroQoL Questionnaire; IVI = Impact of Vision Impairment Questionnaire; IADL = instrumental activities of daily living; IQR = interquartile range.
Figure 1:
The Journal of Blindness Innovation and Research is copyright (c) 2019 to the National Federation of the Blind.